|
The Evolutionary Theory of
Sex:
Congenital
Heart Defects

“Teratological rule of sexual
dimorphism”:
Atavistic anomalies are more frequent in females
while “futuristic” ones occur in males.
Prediction:
According to the theory, female congenital
diseases of the heart and main vessels should carry the
features preserved from the last embryonic stages of
intra-uterine development, or have some attributes peculiar
to a species, from low steps of evolutionary ladder (nearest
past).
The anatomic attributes determining
male's congenital defects should not have precedents
at phylogenetic predecessors of the humans or in the in the
embryo. They are unsuccessful tests of the evolution
process.
Verification:
The prediction was verified by analysis of approximately
32000 congenital malformations of the heart. The most well
defined feminine congenital defects are patent ductus
arteriosus (1♂♂ : 2.72♀♀), Lutembaher disease (1♂♂ : 2.1♀♀),
and ostium
secundum (1♂♂ : 1.84♀♀).
As is known, the arterial channel
makes an integral part of blood circulation of late stages
of development of a fetus and normally gets closed during
the first year after birth. The oval window, which with some
clauses can be identified as atrial septal defect of
secondary type, is the second channel connecting the big and
small circles of blood circulation of a fetus. If closing of
an arterial channel and an oval window does not occur, the
appropriate formations are considered as defects. These
formations as necessary attributes of a structure of adult
normal cardiovascular system can be found at representatives
of the lowest (down to reptiles inclusive) classes of
vertebrata. Thus, these developmental anomalies can be
considered as a return to a near in ontogenetic and
phylogenetic sense to the past, and female prevalence among
ill persons is in agreement with a new rule.
Lutembaher’s disease involves two
components: atrial septal defect (common atrium)
(almost always of secondary type) and a mitral valve
stenosis. First of them, as it was shown, is a congenital
heart disease of a female type. A mitral valve stenosis
related to Lutembaher’s disease is usually an acquired
defect which as is known, at women happens much more often,
than at men. Hence, here there is a combination of two
female components; therefore Lutembaher’s disease is a
typical female heart disease.
For a combination of ventricular
septal defect (neutral defect) and a patent ductus
arteriosus (female defect), presence of a neutral component
brings the ratio down to 1♂♂ : 1.51♀♀, while for the patent
ductus arteriosus only it is equal to 1♂♂ : 2.72♀♀. The
similar picture is observed in the case of Fallot’s triad,
which represents a combination of female defect (common
atrium) with neutral defect (a stenosis of lung artery). The
third component—hypertrophy of right ventricle is not an
independent anatomic formation, but a consequence of the
former two.
Most well defined male's congenital
defects are: congenital aortal stenosis (2.66♂♂ : 1♀♀),
coarctation of aorta (2.14♂♂ : 1♀♀), transpositions of the
great arteries (1.90♂♂ : 1♀♀), total anomalous pulmonary
venous connection (1.39♂♂ : 1♀♀),
and coarctation of aorta with an open
arterial channel (1.37♂♂ : 1♀♀).
No one of male’s components of
congenital heart diseases have a corresponding similar
formation at normal embryo or at phylogenetic predecessors
of the humans.
Other congenital heart defects are of
a neutral type. The frequency of occurrence is about
the same for both sexes. Among them it is also possible to
allocate simple (Potts/Waterston-Cooley shunt and ostium
primum) and complex (partial and full atrioventricular
canal, Ebstain’s anomaly and tricuspid atresia) defects.
Simple defects of this group, as well
as female defects, can be considered atavistic. The
difference between them is that these defects contrary to
female ones represent a return to the past far in
onthogenetic and phylogenetic sense. They can be considered
as consequence of a block in heart development at early
stages of embriogenesis (the first 2-3 months of embryo's
life during which the anatomic formation of the heart
occurs), and on earlier in compare to female defects stages
of Phylogeny.
For complex defects of neutral group
the sex ratio depends on which of their components
prevail—female or male.
The hypothesis presented appears to be more general, than
known
concepts of Rokitansky (1875), Spitzer (1923) and
Krimski (1963) as it explains the genesis not only
female and neutral, but also man's defects. The offered division of congenital
heart diseases and large vessels into male's, female’s
and neutral offers not only theoretical, but also a
certain practical interest. It allows considering sex of
the patient as a diagnostic symptom. This symptom is
stable, cheap and does not harm the patient compare to some
invasive diagnostic procedures.
See the following links for the
pictures of different congenital malformations:
Normal heart:
http://home.cc.umanitoba.ca/~soninr/NormalST.html
Patent ductus arteriosus (F)
http://www.heartpoint.com/congpda.html
Lutembaher disease (F)
Atrial septal defect of secondary type (F)
http://www.heartpoint.com/congasd.html
Combination of ventricular septal defect and a patent ductus
arteriosus (F)
Fallot’s triad (F)
Aortal stenosis (M)
Coarctation of aorta (M)
http://www.heartpoint.com/congcoarct.html
Transpositions of the great
arteries (M)
http://www.heartpoint.com/congtranspos.html
Anomalous
pulmonary venous connection (M)
http://home.cc.umanitoba.ca/~soninr/TAPVC.html
Coarctation of aorta and an open arterial channel (M)
Potts shunt (N)
Waterston-Cooley shunt (N)
Partial and full
atrioventricular canal
Ebstain’s anomaly (N)
http://www.heartpoint.com/congepstein.html
Tricuspid atresia (N)
http://www.americanheart.org/presenter.jhtml?identifier=1310
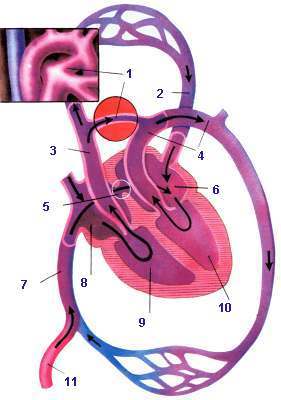 Fetus
blood flow diagram Fetus
blood flow diagram
1. ductus arteriosus
2. pulmonary vein
3. pulmonary artery
4.
aorta
5. foramen ovale
6. left atrium
7. inferior cave vein
8. right atrium
9. right ventricle
10. left ventricle
11. umbilical vessels
Description
As soon as the baby is
born, the foramen ovale, ductus arteriosus,
and umbilical vessels are no longer needed. Within a few days the
ductus arteriosus closes off completely. The Foramen Ovale
closes
gradually over several weeks or months, sometimes remaining
open
as a tiny slit into adolescence or beyond.
See also
http://home.cc.umanitoba.ca/~soninr/NormalST.html
for more details
|